
Viet Le, MPAS PA-C FACC FAHA · @VietHeartPA
100 followers · 1081 posts · Server med-mastodon.com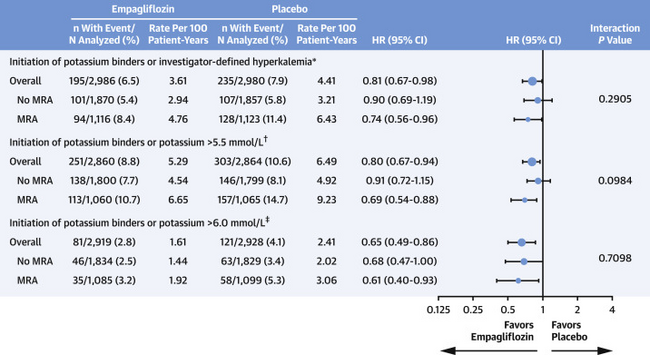
{kind=link}
RT @JJheart_doc
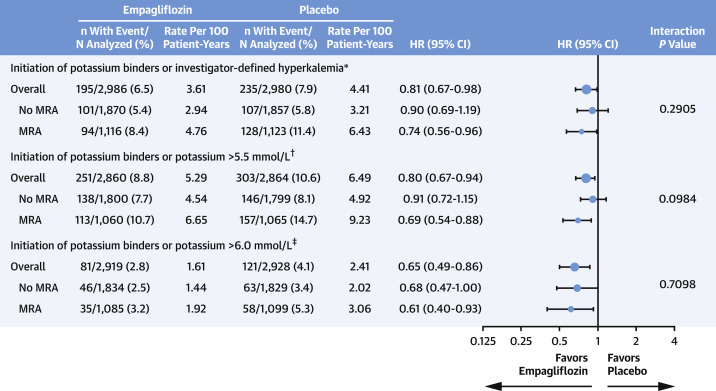
4. Can other #GDMTworks help to preserve use of MRAs? Yes! It was recently shown that use of SGLT2i lead to greater likelihood of persistence on MRA in the EMPEROR program owing to lowering of risk for hyperkalemia. This is from EMPEROR-Preserved:

draashish · @draashish
12 followers · 12 posts · Server med-mastodon.com#STRONGHF showed an 8% absolute risk reduction in the primary end points {The primary endpoint occurred in 15.2% of patients in the high-intensity arm vs 23.1% in the usual care group (hazard ratio, 0.66; 95% CI, 0.50 - 0.86; P = .0021)} Although the benefits are attributed to maximal up-titration of GDMT (w/o SGLT2-I), High-intensity care, post DC, was the key 2 it. Will HealthCare systems make the invstmnt & bolster d talk of outcomes? #MedMastodon #GDMTworks #cardiology #internalmedicine
#stronghf #MedMastodon #gdmtworks #cardiology #internalmedicine
Viet Le, MPAS PA-C FACC FAHA · @VietHeartPA
64 followers · 153 posts · Server med-mastodon.comRT @dranulala
@CardioNerdsJC STRONG-HF Implications for me: #CardsJC
1. High-intensity care = the new and only acceptable Usual Care
2. In hospital initiation of #GDMTworks
3. Follow up every 1-2 weeks after DC until maximal #GDMT achieved
4. Call for strategy based studies on how to implement!
Viet Le, MPAS PA-C FACC FAHA · @VietHeartPA
64 followers · 153 posts · Server med-mastodon.comRT @noshreza
@CardioNerdsJC Still reflecting on a couple of things:
1) ~5% of patients in each arm died w/in 90d & 8-9% died w/in 180d — there is no time to delay in #GDMTWorks!
2) At Day 90, only ~50% of patients w/LVEF <=40% in high-intensity arm were on full dose ACEi/ARB/ARNI or full dose BB