
Real Quack · @ducker
73 followers · 1352 posts · Server union.placeI thought rat #Poison was cumulative - the most common being #Warfarin (which is marketed to humans as a #BloodThinner under brand names such as #Coumadin)
I'm curious how they determined this was occurring.
#poison #warfarin #bloodthinner #coumadin
Simon Lucy · @simon_lucy
248 followers · 691 posts · Server mastodon.socialINR result today 3.1, so that's broken the 12 month run of being well in bounds. Back for another test in a fortnight rather than 6 weeks and dropping a further .5mg over a week. This means the result enters a kind of sinosoidal period until it settles stably within the wanted bounds.
For me this is a normal occurrence but you always get the question is there anything you've done differently?
Simon Lucy · @simon_lucy
257 followers · 767 posts · Server mastodon.socialINR result today 3.1, so that's broken the 12 month run of being well in bounds. Back for another test in a fortnight rather than 6 weeks and dropping a further .5mg over a week. This means the result enters a kind of sinosoidal period until it settles stably within the wanted bounds.
For me this is a normal occurrence but you always get the question is there anything you've done differently?

Autistic Book Club · @autisticbookclub
1342 followers · 1185 posts · Server mastodonapp.uk@linenandspice I was concerned because so many other meds I’ve been on I’ve had an overly sensitive reaction to which happens in our #AutisticCommunity but, unfortunately, it’s not common knowledge amongst doctors🤷♀️
There is a long list of contradictions with #Paxlovid and #Warfarin is one of them, a drug I take. But, there have been no side effects apart from a foul, metallic taste, so be encouraged if you ever must take Paxlovid, but I hope you never have to! 💗
#ActuallyAutistic
#AutisticCommunity #Paxlovid #warfarin #actuallyautistic

Daniel Dvorkin · @medigoth
90 followers · 90 posts · Server qoto.orgEver since the Human #Genome Project got rolling about thirty years ago (!) there’s been a lot of hope, and a lot of hype, about “#personalized #medicine” or “#precision medicine.” When it became clear that as always, the results weren’t going to match the hype, a lot of the hope went away too. This is a mistake.
I’d like to talk about a quiet revolution in precision medicine: #genetic #dosage guidelines, a.k.a. #pharmacogenomic #labeling. The basic idea is that if you carry certain genetic #variants, you may need considerably more or less of a particular medication than the standard dose. Back in the ’90s, the kind of genetic #analysis needed to make use of that information was far too expensive and time-consuming for #clinical practice. These days you can get a complete #sequence in a matter of hours, for the same cost as a battery of standard blood tests.
Fifteen years ago or so, the FDA approved the first pharmacogenomic labeling, for #warfarin. I was lucky enough to be in the room when the researchers made the announcement, and you could have heard a pin drop. Now it’s routine, and there’s a very long list: https://www.fda.gov/drugs/science-and-research-drugs/table-pharmacogenomic-biomarkers-drug-labeling
Everyone reacts to #medications differently. For most patients, most medications, and most diseases, there’s a fairly broad range of clinical effectiveness between “too little to do any good” and “way too much.” But for a substantial number of all of the above, the range is much narrower—and when you add up all the special cases, you get a hell of a lot of people!
A lot of #drugs never get approved, despite showing promise in clinical #trials, because they only help a portion of the study population. Regulatory bodies like the #FDA are notoriously resistant to #subgroup analysis, and I get why: it’s very easy to cherry-pick those subjects in a clinical trial who happen to do well, and then come up with a post hoc explanation for why the test treatment worked for them but not for other participants. Some bad drugs have made it to market because of this kind of chicanery. But of course sometimes there’s a real reason one group does better, and as long as genetic testing is part of the study design from the start, it’s becoming possible to convince regulators that reason is valid.
My work is mostly upstream of this, in the drug #target #discovery phase: finding disease-related #genes and #proteins that might be modifiable with the right medication. Since it’s part of the project from the start, that makes trial design easier, and the results more likely to be accepted. But I’d really like to see more #genomic analysis on drugs that aren’t designed that way too, and I think we’re getting there.
Genetic dosage guidelines, though, are making a real difference in current practice. There are still considerable debates over the merits of many labelings, driven partly by legitimate #statistical concerns and partly by ideology. But the principle is proven beyond reasonable doubt, and it’s saving lives and relieving suffering right now, every day. Much more to come.
#genome #personalized #medicine #dosage #pharmacogenomic #labeling #variants #precision #genetic #clinical #warfarin #medications #drugs #trials #fda #analysis #sequence #subgroup #target #discovery #genes #proteins #genomic #statistical
Daniel Dvorkin · @medigoth
90 followers · 90 posts · Server qoto.orgEver since the Human #Genome Project got rolling about thirty years ago (!) there’s been a lot of hope, and a lot of hype, about “#personalized #medicine” or “#precision medicine.” When it became clear that as always, the results weren’t going to match the hype, a lot of the hope went away too. This is a mistake.
I’d like to talk about a quiet revolution in precision medicine: #genetic #dosage guidelines, a.k.a. #pharmacogenomic #labeling. The basic idea is that if you carry certain genetic #variants, you may need considerably more or less of a particular medication than the standard dose. Back in the ’90s, the kind of genetic #analysis needed to make use of that information was far too expensive and time-consuming for #clinical practice. These days you can get a complete #sequence in a matter of hours, for the same cost as a battery of standard blood tests.
Fifteen years ago or so, the FDA approved the first pharmacogenomic labeling, for #warfarin. I was lucky enough to be in the room when the researchers made the announcement, and you could have heard a pin drop. Now it’s routine, and there’s a very long list: https://www.fda.gov/drugs/science-and-research-drugs/table-pharmacogenomic-biomarkers-drug-labeling
Everyone reacts to #medications differently. For most patients, most medications, and most diseases, there’s a fairly broad range of clinical effectiveness between “too little to do any good” and “way too much.” But for a substantial number of all of the above, the range is much narrower—and when you add up all the special cases, you get a hell of a lot of people!
A lot of #drugs never get approved, despite showing promise in clinical #trials, because they only help a portion of the study population. Regulatory bodies like the #FDA are notoriously resistant to #subgroup analysis, and I get why: it’s very easy to cherry-pick those subjects in a clinical trial who happen to do well, and then come up with a post hoc explanation for why the test treatment worked for them but not for other participants. Some bad drugs have made it to market because of this kind of chicanery. But of course sometimes there’s a real reason one group does better, and as long as genetic testing is part of the study design from the start, it’s becoming possible to convince regulators that reason is valid.
Much of my work is upstream of this, in the drug #target #discovery phase: finding disease-related #genes and #proteins that might be modifiable with the right medication. Since it’s part of the project from the start, that makes trial design easier, and the results more likely to be accepted. But I’d really like to see more #genomic analysis on drugs that aren’t designed that way too, and I think we’re getting there.
Genetic dosage guidelines, though, are making a real difference in current practice. There are still considerable debates over the merits of many labelings, driven partly by legitimate #statistical concerns and partly by ideology. But the principle is proven beyond reasonable doubt, and it’s saving lives and relieving suffering right now, every day. Much more to come.
#medicine #pharmacogenomic #labeling #genome #personalized #precision #genetic #dosage #variants #analysis #clinical #sequence #warfarin #medications #drugs #trials #fda #subgroup #target #discovery #genes #proteins #genomic #statistical
Daniel Dvorkin · @medigoth
90 followers · 90 posts · Server qoto.orgEver since the Human #Genome Project got rolling about thirty years ago (!) there’s been a lot of hope, and a lot of hype, about “personalized medicine” or “precision medicine.” When it became clear that as always, the results weren’t going to match the hype, a lot of the hope went away too. This is a mistake.
I’d like to talk about a quiet revolution in precision medicine: #genetic #dosage guidelines, a.k.a. #pharmacogenomic #labeling. The basic idea is that if you carry certain genetic #variants, you may need considerably more or less of a particular medication than the standard dose. Back in the ’90s, the kind of genetic #analysis needed to make use of that information was far too expensive and time-consuming for #clinical practice. These days you can get a complete #sequence in a matter of hours, for the same cost as a battery of standard blood tests.
Fifteen years ago or so, the FDA approved the first pharmacogenomic labeling, for #warfarin. I was lucky enough to be in the room when the researchers made the announcement, and you could have heard a pin drop. Now it’s routine, and there’s a very long list: https://www.fda.gov/drugs/science-and-research-drugs/table-pharmacogenomic-biomarkers-drug-labeling
Everyone reacts to #medications differently. For most patients, most medications, and most diseases, there’s a fairly broad range of clinical effectiveness between “too little to do any good” and “way too much.” But for a substantial number of all of the above, the range is much narrower—and when you add up all the special cases, you get a hell of a lot of people!
A lot of #drugs never get approved, despite showing promise in clinical #trials, because they only help a portion of the study population. Regulatory bodies like the #FDA are notoriously resistant to #subgroup analysis, and I get why: it’s very easy to cherry-pick those subjects in a clinical trial who happen to do well, and then come up with a post hoc explanation for why the test treatment worked for them but not for other participants. Some bad drugs have made it to market because of this kind of chicanery. But of course sometimes there’s a real reason one group does better, and as long as genetic testing is part of the study design from the start, it’s becoming possible to convince regulators that reason is valid.
Much of my work is upstream of this, in the drug #target #discovery phase: finding disease-related #genes and #proteins that might be modifiable with the right medication. Since it’s part of the project from the start, that makes trial design easier, and the results more likely to be accepted. But I’d really like to see more #genomic analysis on drugs that aren’t designed that way too, and I think we’re getting there.
Genetic dosage guidelines, though, are making a real difference in current practice. There are still considerable debates over the merits of many labelings, driven partly by legitimate #statistical concerns and partly by ideology. But the principle is proven beyond reasonable doubt, and it’s saving lives and relieving suffering right now, every day. Much more to come.
#genome #pharmacogenomic #labeling #genetic #dosage #variants #analysis #clinical #sequence #warfarin #medications #drugs #trials #fda #subgroup #target #discovery #genes #proteins #genomic #statistical

Drug Doctor Jay :verified: · @NeuroDrugDoc
295 followers · 172 posts · Server med-mastodon.com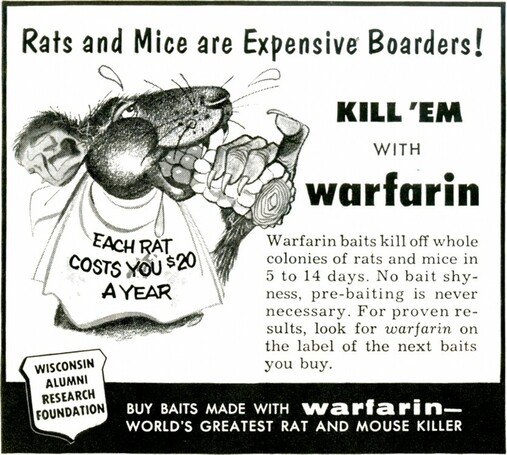
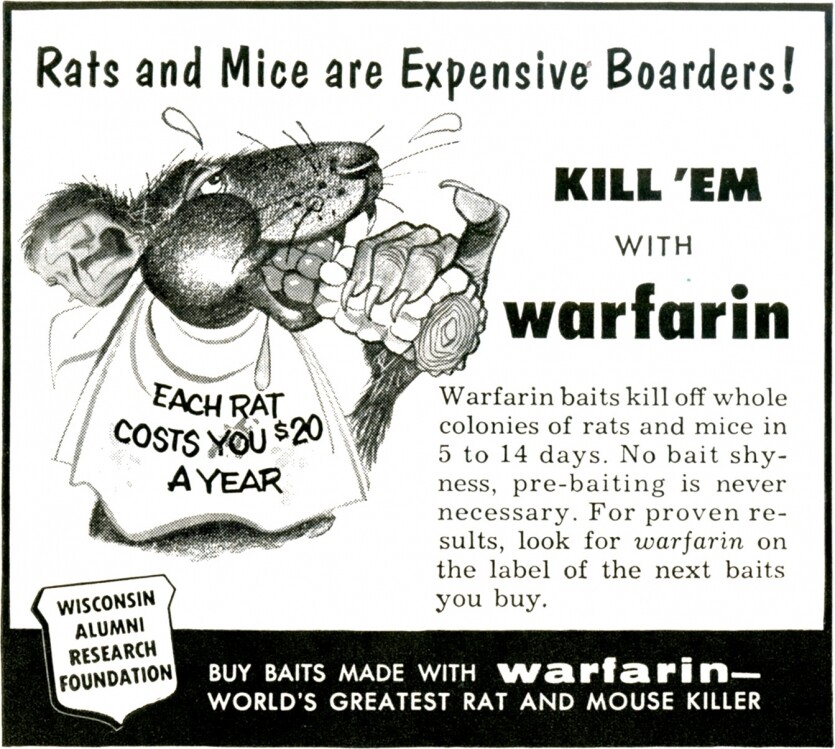
Happy #PharmPhriday! Earlier for #MedicineMonday, I said I’d share more about #warfarin, one of the earliest #anticoagulant drugs.
In the 1920s, there was an outbreak of cattle dying of hemorrhaging after routine procedures. Veterinarians Frank Schofield and Lee Roderick identified moldy silage from sweet clover as the cause. Chemists led by Karl Link identifed the anticoagulating agent, dicoumarin, and further developed it for use as rat poison (1948) then clinically for humans (1954).
#PharmPhriday #MedicineMonday #warfarin #anticoagulant
Drug Doctor Jay :verified: · @NeuroDrugDoc
272 followers · 136 posts · Server med-mastodon.comHope everyone is having a nice start to their week and a smooth transition back for those returning from holiday.
Today’s #MedicineMonday is about #drug names.
🐴 Premarin - pregnant mare urine
6️⃣ Vicodin - 6 (VI) times stronger than codeine
⏱️ Lasix - lasts 6 hours
🐮 Warfarin - WARF (Wisconsin Alumni Research Foundation), arin from coumarin
🩸 Xarelto - Inhibits factor Xa
😴 Ambien - AM, bien (Spanish for “good”)
Any you’d like to add?
More about #warfarin later this week for #PharmPhriday!
#MedicineMonday #drug #warfarin #PharmPhriday

Arya Jaeger · @Arya_Jaeger
7 followers · 547 posts · Server pawoo.net
Arknights Thanksgiving
-
Blue Poison / Ansel / Warfarin / Doctor / Shaw / Manticore / Ifrit / Nearl / Matoimaru / Snowsant
-
#Arknights #Furry #FurryArt #Blue #Frog #Ansel #Bunny #Rabbit #Male #Warfarin #Vampire #Bat #Doctor #Shaw #Squirrel #Manticore #Ifrit #Demon #Nearl #Pegasus #Matoimaru #Oni #Snowsant #Pheasant #Female
#アークナイツ #ケモ #アズリウス #アンセル #ワルファリン #ドクター #ショウ #マンティコア #イフリータ #ニアール #マトイマル #スノーズント
-
https://www.pixiv.net/en/artworks/94529528
-
https://www.deviantart.com/arya-jaeger/art/Arknights-Thanksgiving-899630175
-
https://www.furaffinity.net/view/44882955
#スノーズント #マトイマル #ニアール #イフリータ #マンティコア #ショウ #ドクター #ワルファリン #アンセル #アズリウス #ケモ #アークナイツ #female #pheasant #Snowsant #oni #Matoimaru #pegasus #Nearl #demon #ifrit #manticore #squirrel #shaw #doctor #bat #vampire #warfarin #male #rabbit #bunny #ansel #frog #blue #furryart #furry #arknights
Arya Jaeger · @Arya_Jaeger
7 followers · 547 posts · Server pawoo.net
Arknights - Warfarin Kal'tsit Breeze FEater Manticore
-
#Art #Arknights #Anthro #Furry #FurryArt #Warfarin #Vampire #Bat #Kal'tsit #Cat #CatGirl #Breeze #Fox #FoxGirl #FEater #Panda #PandaGirl #Manticore #ManticoreGirl #Female
#アークナイツ #ワルファリン(アークナイツ) #ケルシー(アークナイツ) #ブリーズ(アークナイツ) #エフイーター(アークナイツ) #マンティコア(アークナイツ)
-
https://www.pixiv.net/en/artworks/89178000
-
https://www.deviantart.com/arya-jaeger/art/Arknights-Line-Up-9-876483646
-
https://www.furaffinity.net/view/41478353
#マンティコア #エフイーター #ブリーズ #ケルシー #ワルファリン #アークナイツ #female #manticoregirl #manticore #pandagirl #panda #feater #foxgirl #fox #breeze #catgirl #cat #kal #bat #vampire #warfarin #furryart #furry #anthro #arknights #art
Arya Jaeger · @Arya_Jaeger
7 followers · 547 posts · Server pawoo.net
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Warfarin
-
#Art #Arknights #Anthro #Furry #FurryArt #Warfarin #Vampire #Bat #Female
#アークナイツ #ワルファリン(アークナイツ)
-
https://www.pixiv.net/en/artworks/88946023
-
https://www.deviantart.com/arya-jaeger/art/Warfarin-875348334
-
https://www.furaffinity.net/view/41332205
#ワルファリン #アークナイツ #female #bat #vampire #warfarin #furryart #furry #anthro #arknights #art